

Related Posts:
- Pulling Through My First Tagging Experience As An Orthopaedic House Officer – Housemanship Diaries
- My Daily Morning Routine As A House Officer In The Orthopaedics Posting – Housemanship Diaries
- The Orthopaedics Posting – Housemanship Diaries
- My “Coming Morning” Priority – Housemanship Diaries
- My Support System During My First Posting In Orthopaedics As A Junior Doctor In Malaysia – Housemanship Diaries
Being a house officer in the emergency & trauma department was one of the enjoyable shifts I’ve ever experienced in the Orthopaedics Posting. It is filled with adrenaline, uncertainties and lots of walking and running here and there. Our shift begins from 7am till 7pm for the morning shift and 7pm till 7am for the night shift, well at least on paper.
For most of my colleagues, they despise working in the ETD/ED. However, personally, I would choose this shift any day over wards. On top of being the medical officer’s / registrar’s assistant, there are a lot of hands-on procedures as well. Hence, it can be such a heavy duty.
The location is of course at the emergency department, in the “POP room” in particular. Well, at least in the hospital that I’m practicing in. The job scope, location and system may differ in other places.
1. EQUIP THYSELF!
Before I proceed into the joblist of an ETD houseman, it is important for you to be well-equipped. The last thing you would want to do is to run from one location to another while the medical officer / registrar / specialist is clerking and examining the patient.
The essential items that I always carry with me are:
A. A Sling Bag

Inside are pens, chop, orange stick, monofilament test, sterile swab for C&S, gloves, tendon hammer, permanent marker and micropore.
B. File

Inside are x-ray forms, KKM forms, MRI consent forms, operation / procedure consent forms, blood consent forms, medication charts and antibiotic charts.
C. Lot of plain papers / continuation sheets on a clipboard
D. My special ETD bag & Doppler

Which consists of blade, gauze (big / small), crepe bandages, green towels and sutures (Nylon 3.0-4.0, Prolene 5.0-6.0), blood tubes, syringes & needles, alcohol swabs and urine bottles (for pus / tissue samples)
Do not forget tons of water and food / bread / snacks and if you are working the night shift, your laptop, adapter and HDMI connector if you are in charge of preparing for handover the following day. These items of course I leave it behind in my main knapsack in the “POP room”. It’s too heavy to be carried around since I am already carrying a bunch of stuffs.
2. WhatsApp

We are extremely “WhatsApp-dependant”. Hence, it is important to ensure that you have excellent internet connection.
Before I proceed to leave for work (if I am the morning shift), I will create a WhatsApp group for the oncall team for that particular day as well as a personal ETD group for myself.
A. Create a WhatsApp Group and rename it as “ETD (Date)”. For example, “ETD 23/10/23-24/10/23”

B. Edit the group description
For example:
- Consultant: (Consultant’s name)
- Surgeon on-call: (Surgeon’s name)
- Tagging specialist on-call: (Specialist’s name)
- Registrar: (Registrar’s name)
- OT: (Medical officer’s name)
- Ward: Medical officer’s name)
- ETD: (Medical officer’s name)
- ETD AM: (House officer-in-charge)
- ETD PM: (House officer-in-charge)
- EMOT AM: (House officer-in-charge)
- EMOT PM: (House officer-in-charge)
- FOW (Female Ortho Ward)
- Tag: (House officer-in-charge)
- SD: (House officer-in-charge)
- LD: (House officer-in-charge)
- ON: (House officer-in-charge)
- MOW (Male Ortho Ward)
- Tag: (House officer-in-charge)
- SD: (House officer-in-charge)
- LD: (House officer-in-charge)
- ON: (House officer-in-charge)
- POW / PSW: (House officer-in-charge)
- Peri: (House officer-in-charge)
- Admission slides: (link)
- Admission list: (link)
I usually prepare this list and create the group the night before. Thus, in the morning, I would just proceed with the rest.
Next, I will then proceed to add the “house officers-in-charge” first into the group and share the link into our “houseman posting group” for others to join. Then, I will proceed to edit the “on-call group name” and description.
For the description, I would copy and paste the same description from the ETD group.
Finally, 5-10 minutes before 7am, I will add the registrar, OT call, ward call and ETD call into the group followed by these 3 messages.

The handover slides and admission list can be obtained from the previous ETD group and it aids the medical officer during passover.
When all of these are settled, it is only THEN, I leave for work. Literally.
I usually leave for work around 6:50 am or 7:00am (as long as it is before 7:30 am, since passover only begins at 7:30 am during weekdays and much later during weekends.)
3. Stock up the “POP Room”
It is our duty as house officers to ensure the “POP room” is stocked and clean. At least for me, I like to keep the area tidy.
Essential items that should be available in abundance in the “POP room”.
- Orthobans (Big ones)
- Crepe bandages
- Forms (i.e: X-ray forms, KKM forms, medication charts, antibiotic charts, operation / procedure consent forms, blood consent forms, MRI consent forms
- Pinkies (those pink absorbable blankets)
- Green towels
- Bedsheets
- Gauze (Big and small)
- Saline for irrigation and drainage
- Blade
- Sutures
- Orange stickes
- Urine bottles for samples
- At least one skin traction
I usually stop by the ward or ETD / ED storeroom to “smuggle” these items for the POP room as well as to leave my knapsack and only then, I will proceed to the “Ortho Clinic” or “Passover Room” for handover, which is at 7:30 am during weekdays an 8am during weekends.
4. Handover & Rounds
The handover is interesting. It is important to have both teams there before commencing which are the post call ETD team from the previous day as well as the on-call team for the day.
The post-call team would present the cases of the admitted patients and usually they will be questioned on their plan / management by the specialists.
Personally, it reminds me of back in medical school where we had to clerk the patient, examine and present a case-based discussion (CBD).
The location of each patient would be updated on the slides itself.

The length of the passover depends on the amount of admissions from the prior day.
After passover is followed by rounds with the current on-call team and post call team as well as the current specialist on call for the day. Only the patients who are “stranded” in the ETD / ED and certain patients upstairs will be seen. Most of the time, it is only within the emergency department.
Thus, what if all patients have been admitted?
Well, no rounds then.
5. Time to STANDBY!
Keep a lookout for the Referral List in the WhatsApp group, which usually gets updated by the ETD call / ward call / Registrar.
In the emergency department, the patients are in green zone (GZ), yellow-zone (YZ) or red zone (RZ).
If the patients are from the green zone, we have to:
- Look for the triage & the patient.
- Bring the patient to the POP room
- Update the name & IC on the referral list
- Upload any x-rays
- Upload wound pictures (with the green background towel)
- Clerk the patient, if you have time
Yellow Zone & Red Zone
- Look for the case-note and identify the patient
- Update the name and IC on the referral list
- Upload any x-rays
- Upload wound pictures (With green background towel)
- Clerk the patient if you have time
Eventually the list gets updated and if you are from the morning shift, you will be carrying out your duties till 7pm after handing over to the person-in-charge at night.
6. Slides & Admission List
In terms of slides & admission list, it is our duty to update all admitted cases, be it under “peri” or “wound” into the slides so the medical officers can present it during handover.
The basic information that needs to be added are:
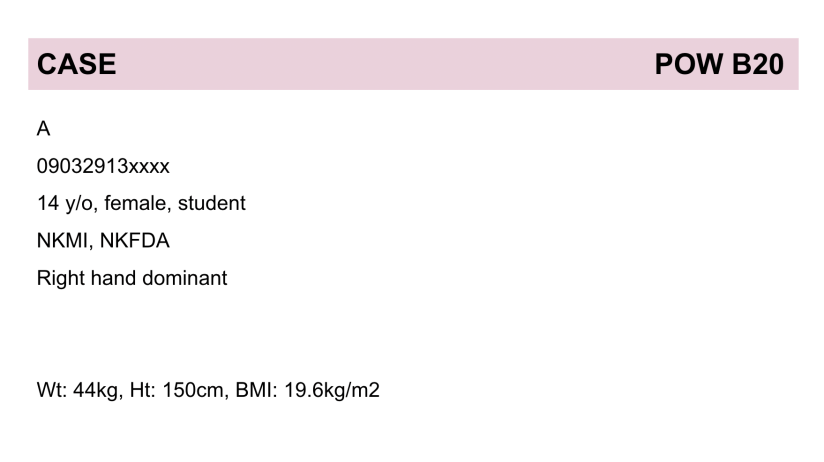
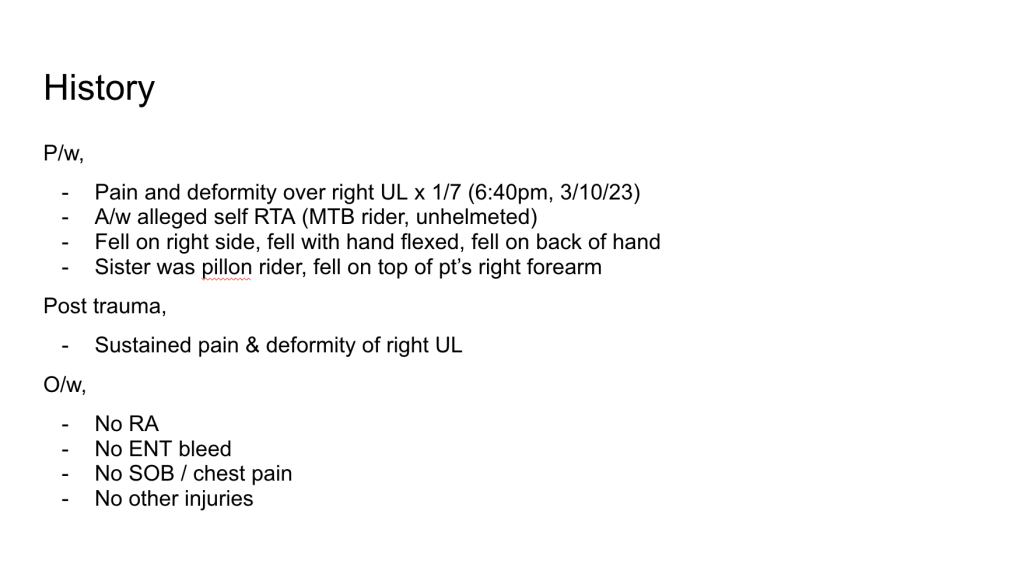



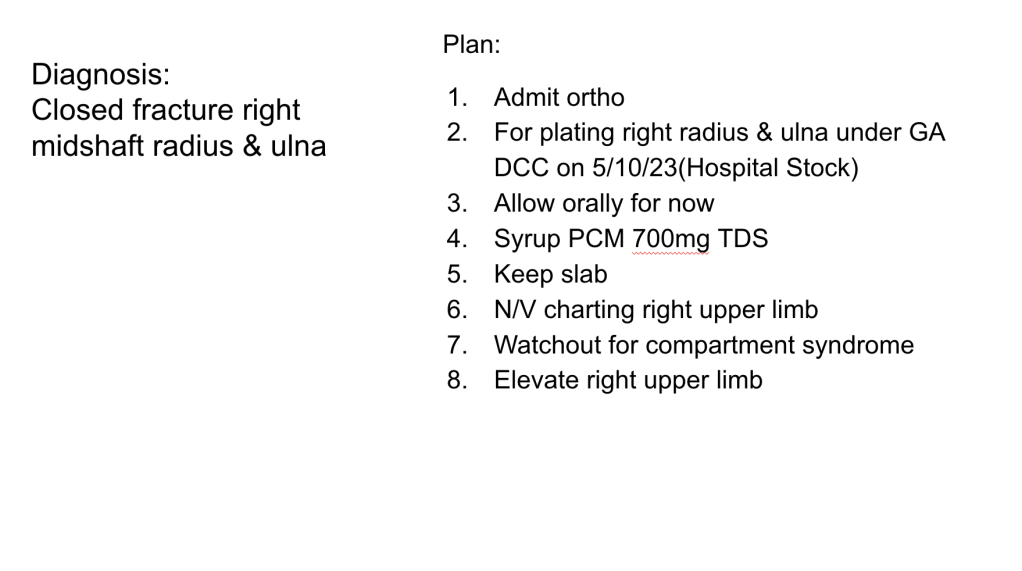
In terms of admission list, the information from the first slide, diagnosis and plan is updated.
Personally, I like to create multiple drafts of the slides beforehand around 15-20 cases, not that I would want that to happen. However, at least, I wouldn’t need to waste extra time copying and pasting just so I can edit them again. It is merely for my convenience.
Being in the emergency department, I learnt that it is very unpredictable, the day/night could be extremely cold, meaning, quiet with 1-2 patients coming in, only to be discharged followed by a trauma alert or a sea of patients flooding in next.
Similarly, the day could be burning with a sea of referrals back to back followed by a cold night with 0-2 admissions.
Or it could be either cold or burning all throughout. The influx of patients on a daily basis varies as well as the variety of cases. It is without a doubt that certain cases are quite common and tends to get boring after some time.
Nevertheless, everyday is still different and special in its own way.
It may take a while for one to adapt or it may be fast. Personally, I have always enjoyed my ETD experience in Orthopaedics and each medical officer provided me with a bunch of things to learn every time and each experience is unique in its own way.
If there is a place that I definitely “come alive”, it would be here followed by in the operating theatre (EMOT).
If you are due to enter the Orthopaedics Posting in your internship / housemanship soon, I wish you all the very best and I hope that the posting is kind to you as it was towards me in addition to learning a bunch of useful and interesting knowledge and procedures.
Related Posts:
- Pulling Through My First Tagging Experience As An Orthopaedic House Officer – Housemanship Diaries
- My Daily Morning Routine As A House Officer In The Orthopaedics Posting – Housemanship Diaries
- The Orthopaedics Posting – Housemanship Diaries
- My “Coming Morning” Priority – Housemanship Diaries
- My Support System During My First Posting In Orthopaedics As A Junior Doctor In Malaysia – Housemanship Diaries
